
Gastric bypass surgery
Roux-en-Y gastric bypass (RYGB), commonly called simply “gastric bypass”, is one of the most commonly performed bariatric procedures worldwide and has long been considered the “gold standard” of bariatric surgery. The gastric bypass was first published in 1967 and was performed as open surgery for several decades. However, since the 1990s, it is almost entirely performed by the laparoscopic (keyhole) approach. The operative procedure involves staple-dividing the stomach into two chambers. The upper chamber – called the pouch – receives food and is very small, holding about 20-30 cc. The lower chamber – called the gastric remnant – is “bypassed” and does not receive food. The small intestine is divided at a certain point and one end is connected (“anastomosed”) to the pouch. A second connection (“anastomosis”) is made to connect the disconnected stomach and duodenum to the small bowel. This connection enables the digestive fluids to meet the ingested food to enable nutrient breakdown and absorption. The distance between the two connections can vary by surgeon preference but is generally 50 to 150 cm. After the procedure is completed, food advances directly from the small gastric pouch to the small intestine without passing through the lower portion of the stomach, duodenum and upper small bowel (jejunum).
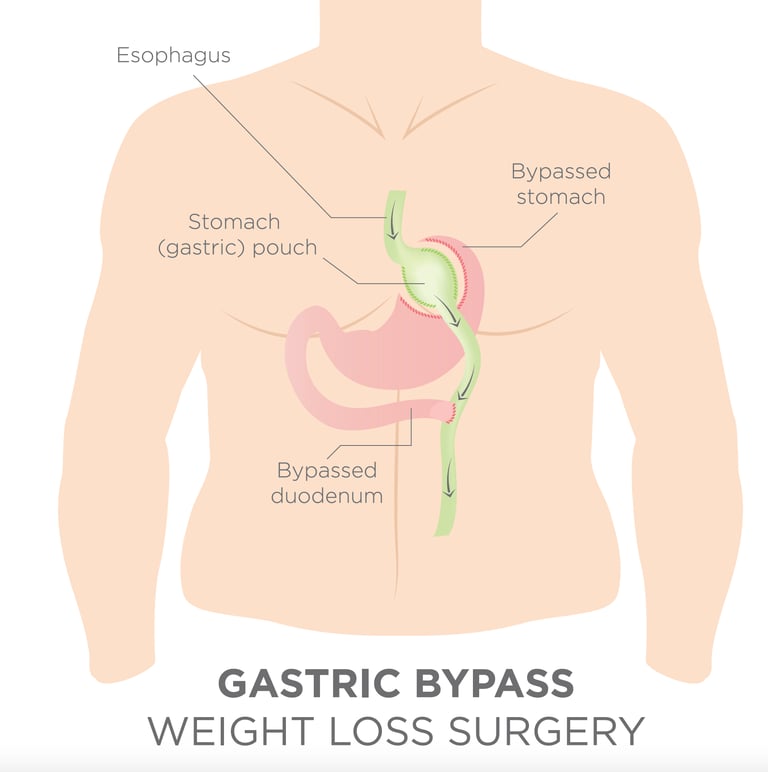
This gastric bypass is thought to help obese people lose weight in several different ways:
The small pouch restricts the amount of food that can be eaten.
The connection between the small bowel and the gastric pouch re-routes the transit of food directly in to the small bowel. Since the food does not go through the bypassed portion of the stomach and duodenum there is less absorption that takes place.
There are further metabolic and hormonal changes that lead to reduced appetite and an increased feeling of fullness.
Following bypass surgery patients can expect to lose around one third of their total body weight or 70 to 75% of the original excess weight. The usual weight loss is 6 kg (1 stone) per month.
The maximum effect on weight loss is normally observed during the first two years. There is typically some weight regained but most studies suggest that most patients maintain a weight loss of around 25% beyond 10 years.
Mr Vasas has a personal experience of more than 1000 primary RYGB procedures (until July 2024) as a primary surgeon, and has zero anastomotic leak and zero mortality. All his operation data is uploaded onto the National Bariatric Surgery Registry and publicly accessible here.


Surgical office
Practice Plus Group's Hospital, Barlborough
2 Limerick Way, Barlborough, Chesterfield, S43 4XE
Contacts
info@bodycontourclinic.co.uk
+44 7794 615316

