
Nissen fundoplication
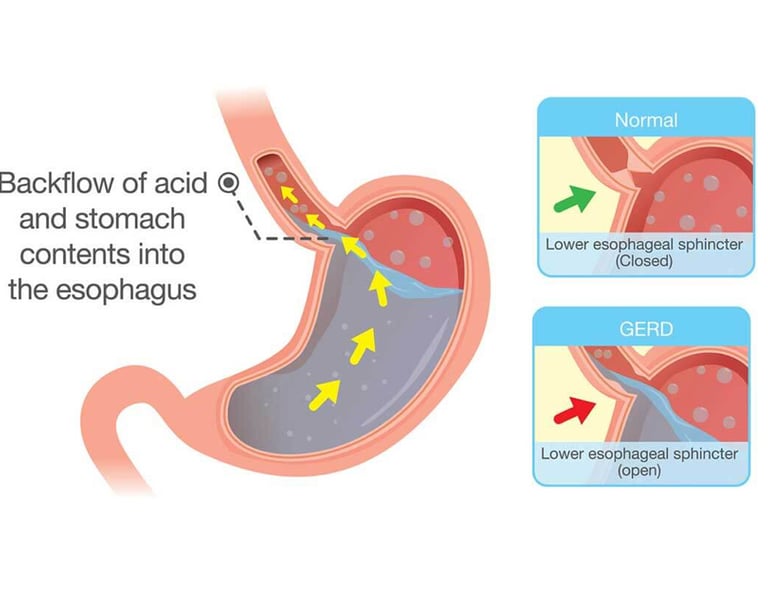
Acid reflux is perhaps the most common gastroenterological disease in developed Western countries, affecting 25-40% of the adult population. The essence of the disease is the reflux of acidic and/or alkaline stomach contents into the esophagus, trachea, or oral cavity. As a result of reflux (abbreviated as GERD or GORD), the mucous membrane of the esophagus can corrode, become inflamed, and even develop an ulcer. Its most characteristic symptom is heartburn, which is an unpleasant pressure, pain or burning sensation behind the sternum. However, reflux symptoms can also occur in the form of coughing, a sore throat, and a dry mouth. If heartburn occurs more often than twice a week, the presence of reflux is likely. In general, the symptoms improve as a result of optimizing lifestyle and diet, but often medication may also be necessary. In appropriate cases, surgical intervention can be performed.
What causes reflux?
Reflux usually occurs when the muscle that closes the lower esophageal section (indicated by the red arrow in the diagram) does not work properly and stomach contents flow into the esophagus. The muscle that closes the lower esophagus is a circular muscle whose role is to prevent the backflow of stomach contents, i.e. it works like a rectifier valve. During swallowing, it "opens", i.e. it allows food to slide down the esophagus, but then it closes and prevents backflow. Diaphragm hernia (hiatus hernia) is often present in reflux patients and very often contributes to the development of reflux symptoms. During this, the upper part of the stomach partially or completely "slips up" into the chest cavity, where the stomach contents flow backwards due to the negative pressure. When acidic (or bilious) stomach contents enter the esophagus, it irritates it and causes heartburn. If the stomach contents are higher, throat irritation, unpleasant tastes, dry mouth and cough (or asthma) may also develop.
What are the symptoms of reflux?
Symptoms caused by reflux can be classified into "typical" and "atypical" groups. Typical symptoms are heartburn and regurgitation of food. Atypical symptoms can be asthma, stubborn cough, hoarseness, nausea, vomiting and large amounts of saliva production at night. Certain foods and medications can significantly worsen reflux symptoms. It is recommended to avoid smoking, pregnancy, obesity, alcohol, caffeine and coffee consumption, fatty foods and carbonated drinks.
What complications can reflux cause?
Acid and/or bile irritates the lower part of the esophagus, which sooner or later can cause damage to the cells of the mucous membrane. The first step is inflammation of the esophagus (oesophagitis), which can range from mild to severe. If the inflammation persists for a long time, bleeding, ulcers, or narrowing of the esophagus (stricture) may occur. Long-term inflammation can also cause permanent damage to the mucous membrane (Barrett's esophagus), which increases the chance of developing a tumor.
How can reflux be treated?
If you notice recurring heartburn or suspect the above symptoms, an internist/gastroenterologist consultation and examination is recommended. First of all, we recommend lifestyle optimization, followed by medication. After that, surgical intervention can be considered.
Lifestyle optimization:
Avoiding foods that cause reflux and enhance symptoms (see above)
Quitting smoking
Eating dinner earlier
Raising the head of the bed at night
Drug treatment:
Antacids (e.g. Gaviscon) are recommended to eliminate heartburn, these are products available without a prescription.
H2 blockers (Ranitidine, Famotidine) can usually reduce the symptoms for a short time, but they require a prescription.
Proton pump inhibitor drugs (Omeprazole, Controloc, Losec) can significantly reduce stomach acid production, but are only available by prescription. Their use for 4-6 weeks significantly reduces the symptoms of reflux, but after stopping them, the return of the symptoms is common. Many patients do not want to take medication for the rest of their lives, which is why they prefer surgery.
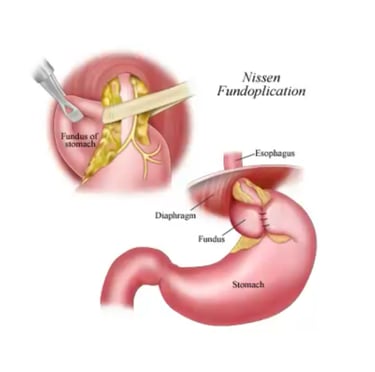
Surgical treatment: Nissen fundoplication.
Reflux can also be treated with minimally invasive surgical methods, during which a cuff is formed from the upper part of the stomach around the lower part of the esophagus. This will act as a valve here, i.e. allowing food to pass through the esophagus, but preventing stomach contents from returning to the esophagus. The intervention takes 60-90 minutes and can be performed through 5 small cuts. After the intervention, it is recommended the patient spends 1 night in the hospital, after which they can go home. After another 10-14 days of recovery, the patients become able to work again, although heavy physical work is not recommended for a further4 weeks.
Who is the surgery recommended for?
those for whom the drug treatment did not bring the expected results
those who can control their reflux symptoms well by taking medication, but do not wish to take medication for the rest of their lives
those who have already developed complications as a result of reflux, such as Barrett's esophagus, ulcer, bleeding, in case of esophageal stricture-atypical symptoms (hoarseness, croaking, asthma)
Advantages of surgery
After the operation, about 90% of the patients are extremely satisfied with the result, and they report that the heartburn has stopped. Reflux-induced asthma and cough improved in about 85% of cases. Barrett's esophagus is not expected to regress as a result of the Nissen operation, but since the corrosive effect of acid-bile does not prevail, the condition usually does not worsen.
Possible complications of surgery
After the operation, almost all patients report temporary difficulty in swallowing, which is inherent to the operation. Therefore, a liquid-paste diet is temporarily recommended for 1-2 weeks, after which patients can return to normal nutrition. The acid-reducing medications you have been taking until then can be omitted. There is a very small chance that difficulty swallowing will require endoscopic dilatation. It is also important to be aware that air swallowed together with food cannot escape through the mouth in all cases (belching is not always possible), therefore abdominal distension may occur, and these gases usually escape through the other end of the alimentary canal. The operation can be safely performed laparoscopically, with a mortality rate of around 0.1%. However, its longer-term complications may include cuff slippage, which results in the loss of the beneficial effects of the surgery.
Dr. Peter Vasas has been performing Nissen fundoplication since 2013. As of October 2022 he has performed 186 such interventions, with a 0% mortality rate. If you think that such an operation can help your reflux disease, please contact us.
Surgical office
Practice Plus Group's Hospital, Barlborough
2 Limerick Way, Barlborough, Chesterfield, S43 4XE
Contacts
info@bodycontourclinic.co.uk
+44 7794 615316

